HAVE YOUR SAY ONLINE: Do you believe that shared decision-making has effective outcomes when implemented in an ob/gyn practice? Have you used it with your patients or have you gone through specific training for it? Let us know what you think by using the hashtag #SDMConvo to tweet to @ContempOBGYN.
Shared decision-making (SDM) is a core element of patient-centered care.Amid increasing calls for SDM in health care, one of the greatest obstacles to implementation may be the fact that many clinicians believe this is their normal practice, when in fact it may not be.
Tina Foster, MD, MPH, MS
Foster is an ob/gyn at the Dartmouth Institute for Health Policy & Clinical Practice and Department of Community and Family Medicine, Geisel School of Medicine at Dartmouth College; she also practices with the Dartmouth-Hitchcock Medical Center, Lebanon, NH.
Rachel C. Forcino, PHD, MSC, Postdoctoral Fellow
Forcino is located at Dartmouth Institute for Health Policy & Clinical Practice and Department of Community and Family Medicine, Geisel School of Medicine at Dartmouth College, Lebanon, NH.
In this article, we describe SDM and discuss approaches to care that may support this process, highlighting ways in which it differs from informed consent and the skills needed to ensure that decision-making is truly shared.
What is shared decision-making?
SDM brings together patient-centered communication and evidence-based medicine to achieve high-quality, patient-centered care.1 The SDM process involves patients and clinicians making decisions collaboratively, informed by the best available scientific evidence as well as each patient’s values and informed preferences.2
There are several important concepts outlined above. “Patient-centered communication” is another widely used but perhaps not universally understood term. Epstein et al.3 define patient-centered communication as:
(1) Eliciting and understanding the patient’s perspective—concerns, ideas, expectations, needs, feelings, and functioning. (2) Understanding the patient within his or her unique psychosocial context. (3) Reaching a shared understanding of the problem and its treatment with the patient that is concordant with the patient’s values. (4) Helping patients to share power and responsibility by involving them in choices to the degree that they wish.3
In the busy world of clinical practice, it can be a challenge to elicit and understand the patient’s perspective as well as her unique psychosocial context. Reaching a shared understanding of both problems and treatments can likewise require time to ensure understanding and to address issues such as health literacy and numeracy.
Finally, in a profession with a long and strong tradition of hierarchy and paternalism, we may struggle with sharing power and responsibility with patients. SDM does not mean ceding all decision-making to the patient, however. Crucially, it incorporates the best available evidence into the decision-making process.
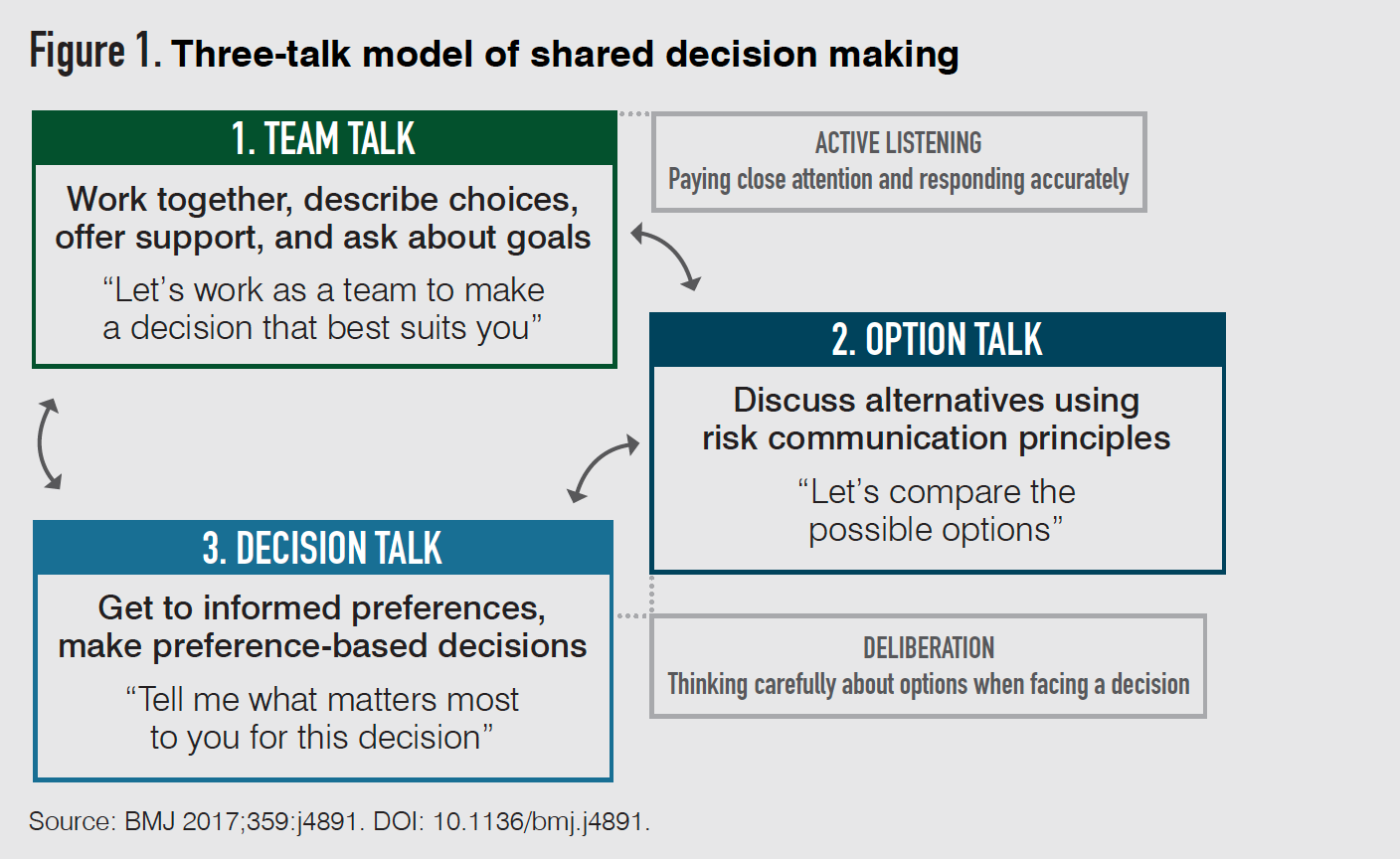
There are a number of frameworks or conceptual models for SDM. The three-talk SDM model2 outlines three steps for clinicians:
- Team talk: Let the patient know that there is a decision to be made, and that you will work together to make a plan focused on her or their individual needs and goals.
- Option talk: Share with the patient high-quality, easy-to-understand information about the benefits and harms of each option under consideration. Consider offering the patient a decision aid to visually compare options.
- Decision talk: Identify the patient’s priorities and plan next steps together according to the patient’s informed preferences.
Informed consent also is described as a means of achieving patient-centered care4 through disclosing information to the patient with her or their subsequent “comprehension, voluntary choice, and authorization” of a procedure or treatment.5
SDM goes a step beyond informed consent, requiring active collaboration in decision-making between patient and clinician.
Patient-centered communication as defined above is clearly central to identifying and understanding patient preferences. While undergraduate and graduate medical education curricula formally address communication skills, these are often neglected with practicing clinicians, unless a clear problem has arisen or “refresher courses” are available.
Even now, SDM may not be part of medical school or residency curricula, so this is a new skill for many. It is likely that many experienced and skilled clinicians could actually benefit from education and coaching related to communication, especially if it includes skills practice.
Many clinicians are surprised to learn that applying the principles of patient-centered communication may not actually increase visit duration.6 Organizations that invest in efforts to develop communication skills of providers often see improvements in patient experience scores and other metrics.
The Academy for Communication in Healthcare is one organization that offers both in-person and online training in relationship-centered communication.
Decision aids can help
Decision aids supplement the information and counseling that is provided directly by clinicians.7 These tools include a description of the decision to be made and balanced, and evidence-based information about the options, including benefits and harms.7 They also help to clarify patients’ values and communicate that the ‘right’ decision depends on the patient’s priorities.7
Decision aids each are designed for a specific treatment or screeningdecision. They are available in multiple formats, including videos, brochures, and web-based tools.7,8
Some decision aids are designed to be used independently by patients outside the health care setting, while others are made for collaborative use by patients and clinicians during a clinic visit.
A variety of decision aids, covering topics like cervical cancer screening, prenatal testing, childbirth, infertility, and uterine fibroids, are available through the Ottawa Hospital Research Institute’s website,9 which also offers helpful materials on how to evaluate the quality of a decision aid.
Additionally, health systems are increasingly subscribing to online decision aid suites that are integrated into their electronic health record systems to facilitate access and use by clinical teams. These tools often have the added benefit of regular updating by an editorial team so that the information presented is up to date.
Patients who use decision aids are better informed about the available options and have a better understanding of what treatment-related priorities matter most to them than those who do not use these tools.7
In ob/gyn, decision aids also have been shown to reduce patients’ decisional conflict, thereby increasing overall comfort with the decision that is made.10
Decision aids used at the point of care
Decision aids are increasingly being designed for use together by patients and clinicians at the point of care.11 Decision aids made for patients’ independent use generally include lengthy explanations of options and exercises to help patients explicitly clarify their values. In contrast, decision aids used at the point of care (often called ‘encounter decision aids’ or ‘conversation aids’) are brief; they provide a basic evidence overview about key aspects of each option in plain language.
These point-of-care decision aids are “not designed to be comprehensive” and rely on clinicians’ “just-in-time, tailored explanations and information.”11 When paired with the three SDM steps outlined above, these aids help to improve deliberation by patients and clinicians without increasing the duration of clinic visits.7
They also provide a framework for the clinician to incorporate patient preferences and values; for example, desire to preserve fertility might frame the choices for fibroid treatment discussed during a visit. Clinicians report becoming comfortable using this type of decision aid with patients after a brief education and minimal practice.12
Implications and future directions
SDM is a cornerstone of patient-centered care,13 and is therefore often considered a moral imperative. However, implementation challenges persist, including competing clinical priorities in clinical workflows and actual practice habits.10
Efforts are currently underway to explore how best to implement SDM in ob/gyn contexts, including ensuring that decision aids are provided to the right patients at the right time in their decision-making processes.14 Inclusion of online decision aids in electronic health records is one promising approach under exploration.
In other contexts, sweeping policy-level implementation efforts have mandated SDM. The Centers for Medicare and Medicaid Services, the largest healthcare payer organization in the United States, now requires documentation of SDM using a high-quality decision aid as a prerequisite to payment for lung cancer screening,15 implantable cardioverter-defibrillator implant,16 and left atrial appendage closure.17
It is unknown whether future SDM mandates will impact the ob/gyn practice, but given the many relevant decisions our patients face (genetic screening, medical vs. surgical abortion, trial of labor after cesarean, management of pelvic organ prolapse, et cetera), they may be on the horizon.
More importantly, it is our obligation to provide the best evidence while working to understand our patients’ values, preferences, and context.
While SDM is critical to patient-centered care, it is not yet universal in care or training in ob/gyn. As there are many opportunities for SDM in ob/gyn, it will be important for trainees and practicing providers to understand the principles of SDM, learn skills that support patient-centered communication, and become familiar with and develop new decision aids.
Takeaways
- Patient-centered communication includes: 1) eliciting and understanding the patient’s perspective; 2) understanding the patient within her or their unique psychosocial context; 3) reaching a shared understanding of the problem and treatment that is concordant with the patient’s values; and 4) helping patients to share power and responsibility by involving them in the choice to be made.
- SDM requires that clinicians: 1) identify that there is a decision to be made; 2) share evidence-based information about the benefits and harms of each potential option; and 3) plan next steps together according to the patient’s informed preferences.
- Using decision aids as part of an SDM process at the point of care improves decision-making outcomes without increasing clinic visit duration.
- Clinicians and patients report ease of use and satisfaction with point-of-care decision aids.
References
- Hoffmann TC, Montori VM, Del Mar C. The connection between evidence-based medicine and shared decision making. JAMA. 2014;312(13):1295-1296.
- Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891.
- Epstein RM, Franks P, Fiscella K, et al. Measuring patient-centered communication in Patient–Physician consultations: Theoretical and practical issues. Social Science & Medicine. 2005;61(7):1516-1528. doi:10.1016/j.socscimed.2005.02.001.
- Krumholz HM. Informed consent to promote patient-centered care. JAMA. 2010;303(12):1190-1191.
- Grady C. Enduring and emerging challenges of informed consent. N Engl J Med. 2015;372(9):855-862.
- Laws MB, Epstein L, Lee Y, et al. The association of visit length and measures of patient-centered communication in HIV care: A mixed methods study. Patient Educ Couns. 2011;85(3):e183-e188.
- Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4:CD001431.
- Drug and Therapeutics Bulletin. An introduction to patient decision aids. BMJ. 2013;347:f4147.
- Ottawa Hospital Research Institute Decision Aid Inventory. Accessed August 25, 2020. https://decisionaid.ohri.ca/AZlist.html.
- Poprzeczny AJ, Stocking K, Showell M, Duffy JMN. Patient Decision Aids to Facilitate Shared Decision Making in Obstetrics and Gynecology. Obstetrics & Gynecology. 2020;135(2):444-451. doi:10.1097/aog.0000000000003664.
- Agoritsas T, Heen AF, Brandt L, et al. Decision aids that really promote shared decision making: the pace quickens. BMJ. 2015;350:g7624.
- Elwyn G, Rasmussen J, Kinsey K, et al. On a learning curve for shared decision making: Interviews with clinicians using the knee osteoarthritis Option Grid. J Eval Clin Pract. 2018;24(1):56-64.
- Barry MJ, Edgman-Levitan S. Shared decision making—pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780-781.
- Scalia P, Durand M-A, Forcino RC, et al. Implementation of the uterine fibroids Option Grid patient decision aids across five organizational settings: a randomized stepped-wedge study protocol. Implement Sci. 2019;14(1):88.
- Decision Memo for Screening for Lung Cancer with Low Dose Computed Tomography (LDCT) (CAG-00439N). Accessed August 25, 2020. https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=274
- Decision Memo for Implantable Cardioverter Defibrillators (CAG-00157R4). Accessed August 25, 2020. https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=288
- Decision Memo for Percutaneous Left Atrial Appendage (LAA) Closure Therapy (CAG-00445N). Accessed August 25, 2020. https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=281