






Have no fear! Premenarchal vaginal bleeding
Part 1 in a series on emergencies in pediatric and adolescent gynecology.
Gynecologic conditions that are common in girls and adolescents are often not seen in adult patients or can present differently, creating a dilemma for the provider.1 Because these are relatively rare occurrences, this review is designed to guide a general obstetrician-gynecologist through several case-based scenarios of premenarchal vaginal bleeding. These scenarios are intended to give the general gynecologist guidance, but consultation with or referral to a pediatric and adolescent gynecologist in an academic medical center may be indicated.
Case 1: A 4-year-old presents with 1 day of spots of blood in her underwear that the mother noticed when helping her daughter change. The child denies any falls; does not complain of pain, dysuria, or itching; and has been supervised by her mother all day. See Figure 1 for her exam. What is your diagnosis?


Figure 1

Discussion: In this patient, the exam shows whitening of her vulva (classically, in a “figure of 8” distribution that can surround the anus) in addition to several areas of subepithelial hemorrhage (“blood blisters”) and scarring around the clitoral hood, consistent with lichen sclerosus (LS)—a chronic inflammatory skin disease that primarily presents in the anogenital region. It most commonly affects females and may occur premenarche or after menopause, likely due to lower estrogen levels.2 The disease is estimated to occur in 1 in 900 prepubertal girls.3 The pathogenesis of LS is multifactorial and can be associated with other autoimmune conditions including thyroiditis, alopecia, pernicious anemia, and vitiligo.4 Occasionally, LS may look like significant bruising and has been mistaken for abuse.5 The whiteness of the surrounding skin and the presence of scarring should alert the provider to the correct diagnosis.6 Although the association of vulvar cancer has been made in adults, this has not been described in children. Treatment is indicated to alleviate symptoms—usually itching or pain—and to prevent further scarring. Ultrapotent topical corticosteroids are often used initially with tapering to lower-potency ointment for maintenance; tacrolimus may be used as second-line therapy.6
It is important to note that, besides trauma-related bleeding (both accidental and nonaccidental/abuse), most of the possible reasons for premenarchal vaginal bleeding are not true emergencies; however, they often present as such due to anxiety in the patient
and caregiver.7


Table
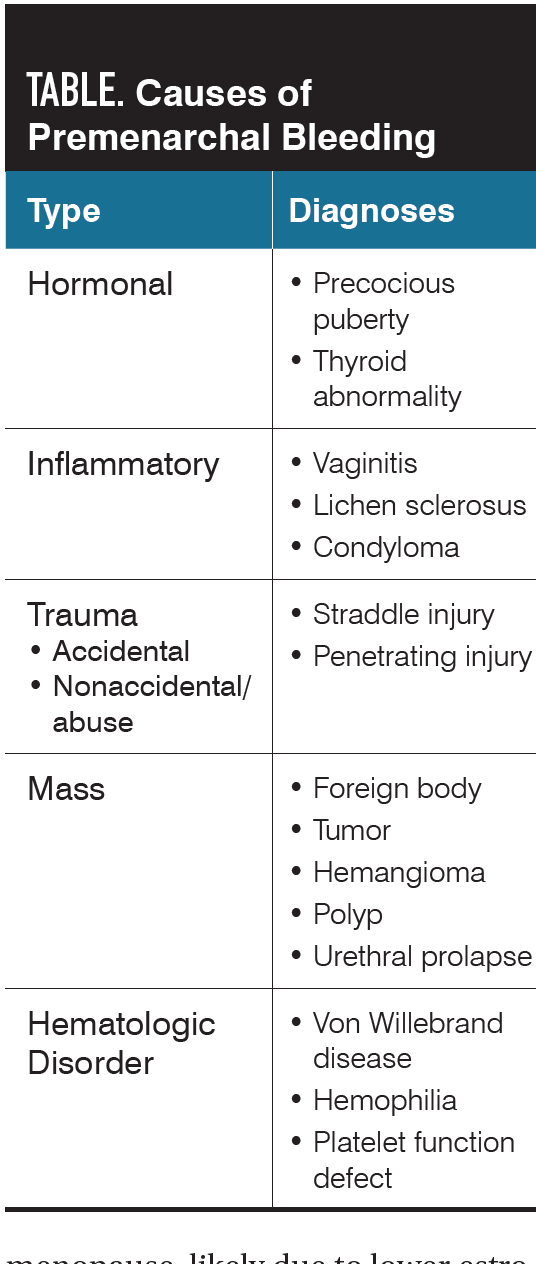
The differential diagnosis list for premenarchal vaginal and vulvar bleeding is long (Table), with trauma and precocious puberty as the diagnoses that initially need to be ruled out. Vulvar concerns and urologic factors are the most encountered etiologies.8
The physical exam of the premenarchal girl who presents with bleeding should always include a breast exam, as any breast development prior to age 7 is cause for concern for precocious puberty.
After an abdominal exam, a vulvar exam should be attempted. This can be more complicated than it would be in an adolescent or adult patient. First, the provider must explain the plan to the patient and parent, including that only an external exam will likely be performed. A speculum examination of a prepubertal girl in the office is never indicated. For a very anxious girl, it is helpful to consider having a child life specialist at the exam if feasible.
The child should sit in a lithotomy position, either on the parent’s lap or in frog-leg position on the exam table, with the desired parent or caregiver by her side. Stirrups are usually not used, as this can make the child uncomfortable. Gentle, lateral traction on the labia majora should be used for vulvar visualization. Gently gripping the labia majora and pulling anteriorly allows the edges of the hymen to be seen.9 Deep breathing should be encouraged, as this helps to open the vagina and further enables the hymenal edges to be more easily appreciated.4 The child should always be informed of the examiner’s actions prior to every maneuver.
If there is a need to look deeper into the vagina or if the child is more comfortable on her abdomen, the child can lie in a prone knee-chest position. In this position, the child lies on her knees with her buttocks elevated and her head resting on the table. Her arms can be positioned above her head or by her side. An otoscope can be used to see inside the lower vagina. Topical lidocaine jelly may be helpful with this exam.


Figure 2
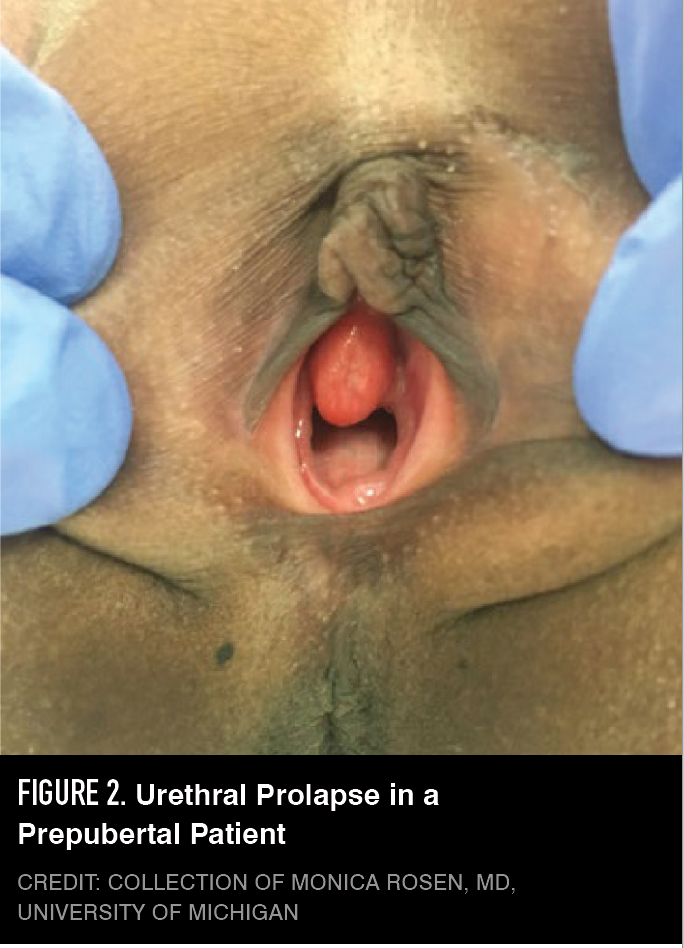
With a similar story but different exam, this patient could also have had a urethral prolapse (Figure 2), which has an incidence of 1 in 3000 premenarchal girls.10 The most common presentation is vaginal bleeding, as the prolapsed tissue can be friable; pain may also occur.11 This happens when there is a lack of urethral support, enabling the urethral mucosa to prolapse and form a friable mass, and is more common in Black girls. The distinction between urethral prolapse and a vaginal mass or tumor can be facilitated by observing the child voiding on a bedpan; urine exits through the center of the prolapsed urethra, and anterior to a vaginal mass. Sitzbaths and topical estrogen are the mainstays of treatment; surgical intervention is rarely necessary if necrosis is present.10
Case 2: A 5-year-old girl presents with foul-smelling bloody vaginal discharge that she has had for 1 week. Based on a normal vulvar exam, except for purulent discharge, you diagnose vulvovaginitis and treat her with oral antibiotics for 7 days. The discharge disappears but returns when the antibiotic course is complete. What is the most likely diagnosis and treatment?
Discussion: When discharge persists despite antibiotics, there is suspicion for a foreign body. Foreign bodies occur in up to 18% of girls with bleeding and discharge.12 Until the foreign body is removed, the discharge or bleeding will likely continue. The most common foreign body is toilet paper, although all manner of objects may be intentionally placed in the vagina by the child. It may be hard to see the foreign body in clinic on the exam, even in a knee-chest position. If the foreign body can be easily seen at the introitus, it can be carefully removed with a small instrument. A rectal exam may aid in palpating a firm object, and the object can sometimes be removed by “milking” it toward the introitus. Again, lidocaine jelly may be helpful.
Options for removal of a deeper or nonvisible foreign body include a lavage or irrigation in an office setting, office vaginoscopy or irrigation with an office hysteroscope (Endosee; CooperSurgical). This choice is based on patient anxiety, tolerance of the initial examination, and family preference. If the decision is a clinic lavage, child life assistance can be invaluable. Before performing a lavage, the gynecologist can apply topical lidocaine jelly to the hymen for comfort. With the patient in a frog-leg position, a small pediatric feeding tube or foley is attached to a 20-mL syringe of warm saline. The catheter tube is passed through the hymenal opening and irrigation of the vagina is initiated. Some water pressure may be required to help loosen the foreign body. During irrigation of the vagina, touching the hymen should be avoided. A small foreign object may exit the vagina with this technique.13


Figure 3
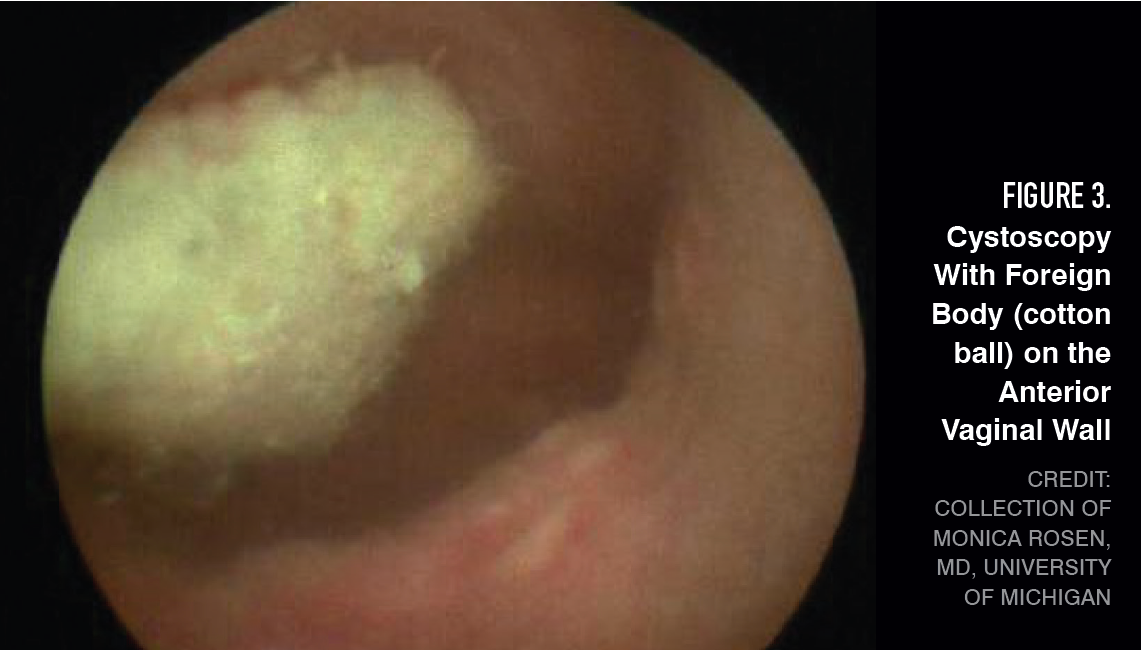
If an office exam is not desired, pelvic imaging can be obtained, although this does not always show the foreign body.14 A vaginoscopy under general anesthesia using a pediatric cystoscope can be performed to better visualize the vagina and the foreign body. With vaginoscopy, the labia majora can be held closed to allow for vaginal distension and better visualization. Common culprits are toilet paper or cotton balls (Figure 3).
Remark: With premenarchal vaginal bleeding, it is important to remember a rare reproductive system malignancy: embryonal rhabdomyosarcoma—also known as sarcoma botryoides.15 This malignancy involves the vagina, uterus, bladder, and urethra and typically presents with the passage of grape-like lesions and/or vaginal bleeding or discharge. Ninety percent of these tumors occur before a child turns 5 years of age, with most occurring before age 2. Growth is rapid and treatment involves a combination of surgery, chemotherapy, and radiation, decided upon using a multidisciplinary team approach.16 Fortunately there are high cure rates, so early detection is imperative.
You are paged urgently to the emergency department to see an 8-year-old girl who reports falling on the side of the bathtub an hour ago. She reports pain in her genital area after straddling the tub, along with some vaginal spotting. What do you do next?
Discussion: This girl has suffered a straddle injury. Straddle injuries are the most common gynecologic injury in this age group and are usually the result of blunt trauma,17 which occurs when soft tissue is compressed against bone, causing bruising and superficial lacerations. Hymenal involvement
is rare.
In this case, the provider should first assess the patient’s stability, then take a history. There may be concern for nonaccidental trauma, so this should include the exact circumstances of how the trauma occurred and if it was witnessed. If possible, the provider should interview the child alone if she is of an appropriate age. On examination of the vulva, it is important to specifically evaluate whether the injury fits the history that was given. The hymen should be assessed to see if it is involved. In a typical straddle injury on a nonsharp surface, a hymenal laceration is uncommon; therefore further evaluation of the circumstances of this trauma must occur, possibly with the help of a child protection team or social worker.
In findings from recent studies, 1 in 5 girls are estimated to experience sexual abuse during childhood.19 It is important to remember, however, that most children who are evaluated for suspected sexual abuse will not have any signs of injury; minor injuries can heal quickly, and bruising, abrasions, and lacerations are rare in children examined more than 72 hours after experiencing abusive trauma.18
If there is significant bleeding, irrigating with warm water may help delineate the extent of the trauma. Applying topical lidocaine prior to the exam can also be helpful, although it may sting on an open wound. An exam under anesthesia with possible vaginoscopy should be considered for any of the following: the patient is unable to tolerate an exam, vital signs are unstable, the extent of the injury or laceration cannot be appreciated at the bedside, there is active bleeding, or the pain is not responding to appropriate measures.
This patient’s hymen was annular and no hymenal tear or injury was noted. She had a small laceration below the labium minus that became hemostatic without repair. In this instance, her injury fit her history, her parents had observed her accident, and abuse was not suspected. Treatment was supportive, as she did not require a laceration repair. An ice pack applied intermittently may be helpful; a package of frozen food, such as peas, can be wrapped in cloth and will conform to the vulvar area.
Conclusion
Although patients and caregivers often perceive the cases described above as true crises, many such patients may present to a general obstetrician-gynecologist in an office setting. When performing an exam on children, having them adopt the frog-leg or knee-chest position can reduce their anxiety and make them feel more at ease. When in doubt, consider consulting with a gynecologist experienced in pediatric gynecology.
References
1. Roos EJ, Simms-Cendan J, Cheung C, Laufer D, Grover SR; FIGIJ board in collaboration with FIGO. Pediatric and adolescent gynecology through a global lens. Int J Gynaecol Obstet. 2022;156(2):189-196. doi:10.1002/ijgo.13723
2. Powell JJ, Wojnarowska F. Lichen sclerosus. Lancet. 1999;353(9166):1777-1783. doi:10.1016/s0140-6736(98)08228-2
3. Powell J, Wojnarowska F. Childhood vulvar lichen sclerosus: an increasingly common problem. J Am Acad Dermatol. 2001;44(5):803-806. doi:10.1067/mjd.2001.113474
4. Murphy R. Lichen sclerosus. Dermatol Clin. 2010;28(4):707-715. doi:10.1016/j.det.2010.07.006
5. Simms-Cendan J, Hoover K, Marathe K, Tyler K. NASPAG clinical opinion: diagnosis and management of lichen sclerosis in pediatric and adolescent patients. J Pediatr Adolesc Gynecol. 2022;35(2):112-120. doi:10.1016/j.jpag.2021.09.008
6. Alaniz VI, Rosen M, Mohr B, Markman L, Quint EH. 4-year-old girl · genital discomfort and dysuria · clitoral hood swelling · blood blister on the labia minora · Dx? J Fam Pract. 2019;68(5):E8-E10.
7. Craighill MC. Pediatric and adolescent gynecology for the primary care pediatrician. Pediatr Clin North Am. 1998;45(6):1659-1688. doi:10.1016/s0031-3955(05)70107-3
8. Fishman A, Paldi E. Vaginal bleeding in premenarchal girls: a review. Obstet Gynecol Surv. 1991;46(7):457-460. doi:10.1097/00006254-199107000-00016
9. French A, Emans SJ. Office evaluation of the child and adolescent. In: Emans SJ, Laufer MR, DiVasta A, eds. Emans, Laufer, Goldstein’s Pediatric and Adolescent Gynecology. 7th ed. Lippincott Williams & Wilkins; 2019:3-22.
10. Ballouhey Q, Galinier P, Gryn A, Grimaudo A, Pienkowski C, Fourcade L. Benefits of primary surgical resection for symptomatic urethral prolapse in children. J Pediatr Urol. 2014;10(1):94-97. doi:10.1016/j.jpurol.2013.06.011
11. Fernandes ET, Dekermacher S, Sabadin MA, Vaz F. Urethral prolapse in children. Urology. 1993;41(3):240-242. doi:10.1016/0090-4295(93)90565-r
12. Striegel AM, Myers JB, Sorensen MD, Furness PD, Koyle MA. Vaginal discharge and bleeding in girls younger than 6 years. J Urol. 2006;176(6 Pt 1):2632-2635. doi:10.1016/j.juro.2006.08.056
13. Smith YR, Berman DR, Quint EH. Premenarchal vaginal discharge: findings of procedures to rule out foreign bodies. J Pediatr Adolesc Gynecol. 2002;15(4):227-230. doi:10.1016/s1083-3188(02)00160-2
14. Nayak S, Witchel SF, Sanfilippo JS. Vaginal foreign body: a delayed diagnosis. J Pediatr Adolesc Gynecol. 2014;27(6):e127-129. doi:10.1016/j.jpag.2013.10.006
15. Pommert L, Bradley W. Pediatric gynecologic cancers. Curr Oncol Rep. 2017;19(7):44. doi:10.1007/s11912-017-0604-7
16. Strickland AL, Fadare O. Pediatric vulvar malignancies: rare but important to know. Semin Diagn Pathol. 2021;38(1):99-109. doi:10.1053/j.semdp.2020.09.001
17. Spitzer RF, Kives S, Caccia N, Ornstein M, Goia C, Allen LM. Retrospective review of unintentional female genital trauma at a pediatric referral center. Pediatr Emerg Care. 2008;24(12):831-835. doi:10.1097/PEC.0b013e31818ea064
18. Berenson AB, Heger AH, Hayes JM, Bailey RK, Emans SJ. Appearance of the hymen in prepubertal girls. Pediatrics. 1992;89(3):387-394.
19. Adams JA. Sexual abuse in children: what the general practice ob/gyn needs to know. Clin Obstet Gynecol. 2020;63(3):486-490. doi:10.1097/GRF.0000000000000539
Newsletter
Get the latest clinical updates, case studies, and expert commentary in obstetric and gynecologic care. Sign up now to stay informed.

















