Can technology help provide answers to a complex condition? This guide demonstrates how to use ultrasound as a first-line diagnostic tool.
Can technology help provide answers to a complex condition? This guide demonstrates how to use ultrasound as a first-line diagnostic tool.
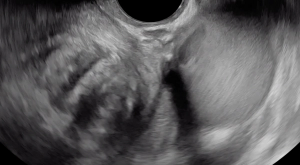
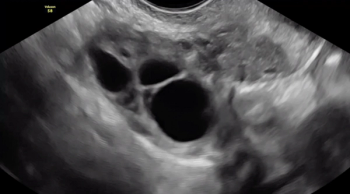
In this clip, fluid within the rectouterine pouch introduced following saline-infusion sonoPODography allows for appreciation of adhesions and a peritoneal pocket (enclosed fluid due to a defect in the peritoneum). These are two classic features of superficial endometriosis.
Although not clearly depicted in this clip, deep endometriosis likely is present posterior to the uterus at the level of the internal cervical os, as demonstrated by the irregular, hypoechoic area.

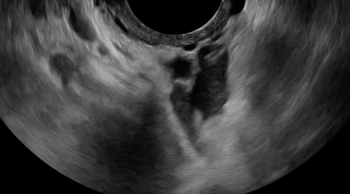
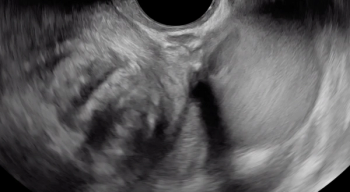
The uterine fundus is being pushed cephalad by the transvaginal ultrasound probe, eliciting smooth sliding of the uterine fundus over the bowel. Some fluid is noted within the rectouterine pouch, which often suggests a non-obliterated pouch.

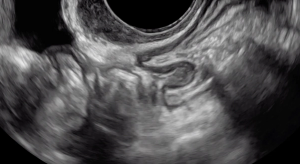
In this case, there is a fixed ovary posteriorly and subtle hypoechoic nodule posterior to the uterus at the level of the internal cervical os, suggesting of deep endometriosis of the torus uterinus.

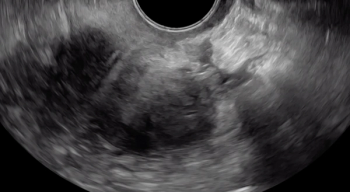
Pressure is being applied to the uterus by the ultrasound operator’s non-scanning hand, eliciting smooth sliding of the posterior uterine serosa over the bowel. Some fluid is noted within the rectouterine pouch, which often suggests a non-obliterated pouch

A hypoechoic deep endometriosis nodule is noted within the hyperechoic uterosacral ligament, infiltrating the parametrium

A hypoechoic deep endometriosis nodule is noted within the hyperechoic uterosacral ligament.

A hypoechoic deep endometriosis nodule is noted within the hyperechoic uterosacral ligament. In this case, there is an ovary containing an endometrioma fixed to the uterosacral ligament nodule.

The beginning of the clip depicts a thin hyperechoic layer just deep to the vagina, which represents the rectouterine pouch peritoneum.

Following the hypoechoic layer of the bowel wall throughout the clip, viewers can appreciate the consistency of the thickness and echogenicity of this layer.

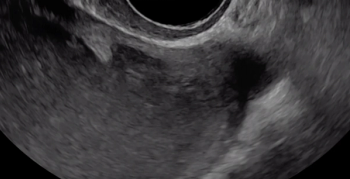
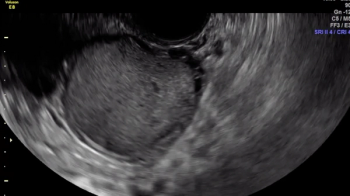
Large rectal deep endometriosis nodule completely fixed to the fundus of a retroverted, retroflexed uterus, resulting in complete rectouterine pouch obliteration (negative sliding sign).

Viewers should focus their eyes on the area closest to the probe, the vagina. With the application of pressure, the operator is attempting to understand whether the bowel is tethered, which it is (demonstrated by the acute angle of the rectal wall muscularis being pulled toward the area of the deep endometriosis nodule).
Viewers should focus their eyes on the area closest to the probe, the vagina. The hypoechoic area that is immediately abutting the probe is consistent in thickness and echogenicity throughout the sweep from right to left. There is other deep endometriosis in this clip (bowel and uterosacral ligament) and an ovarian endometrioma.
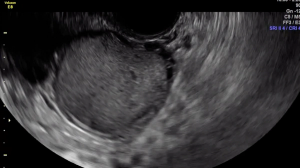
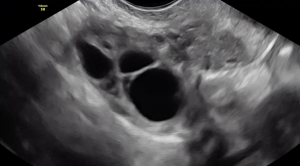
In transverse, this clip shows the right and left ovary both contain an endometrioma and the ovaries are fixed to each other medially, known as “kissing ovaries.” They are densely adherent to an area that also contains bowel deep endometriosis.
Allowing your eyes to follow the external contours of the ovary, it is possible to appreciate the ovary is mobile laterally and inferomedially.
The left side of the ovary (when watching the video) is noted to be densely fixed to an area of deep endometriosis within the uterosacral ligament that is in close proximity the uterus.
The right side of the ovary (when watching the video) is noted to slide smoothly over the pelvic sidewall laterally, suggesting that it is mobile in this dimension.
March 1st 2020
March 1st 2020
March 1st 2020

March 1st 2020
March 1st 2020